
Yesterday, I posted a piece examining the oft-quoted mortality rate for measles of one to two deaths per thousand cases of infection. Today, I want to look at what can be learned from more recent and more comprehensive dataset – this one from the 2008-2011 measles outbreak in France.
In the early 2000’s, measles was a relatively rare occurrence in France. From 2008 to 2011 though, there was a dramatic increase in cases – peaking at over 3,000 new cases per month being recorded in 2011. Because the outbreak occurred in a developed country where the disease was no longer considered a pressing pubic health issue, it provides a unique opportunity to estimate mortality rates following infection by the virus in economies with robust healthcare systems.
In 2013, Denise Antona and co-authors published a comprehensive assessment of the outbreak in the Centers for Disease Control and Prevention journal Emerging Infectious Diseases. Over the four year study period, there were 22,178 documented cases of measles. 11.6% of cases (2,582) involved complications , including pneumonia (1,375 cases, 6.2%), acute otitis media (321 cases, 1.4%), and hepatitis or pancreatitis (248 cases, 1.1%). According to the paper’s authors, diarrhea was reported in 100 cases (0.4%). Overall, there were ten deaths reported (0.05%).
The data are particularly useful for examining morbidity and mortality rates associated with measles in a developed country like France, as with the relative novelty of the disease, the number of reported cases is likely to have been substantially higher than in earlier decades when the disease was commonplace.
In table 1 below (based on Antona et al.’s paper), the number of measles-related complications per 10,000 cases of infection is given for different health impacts and age ranges, based on individuals who were hospitalized.
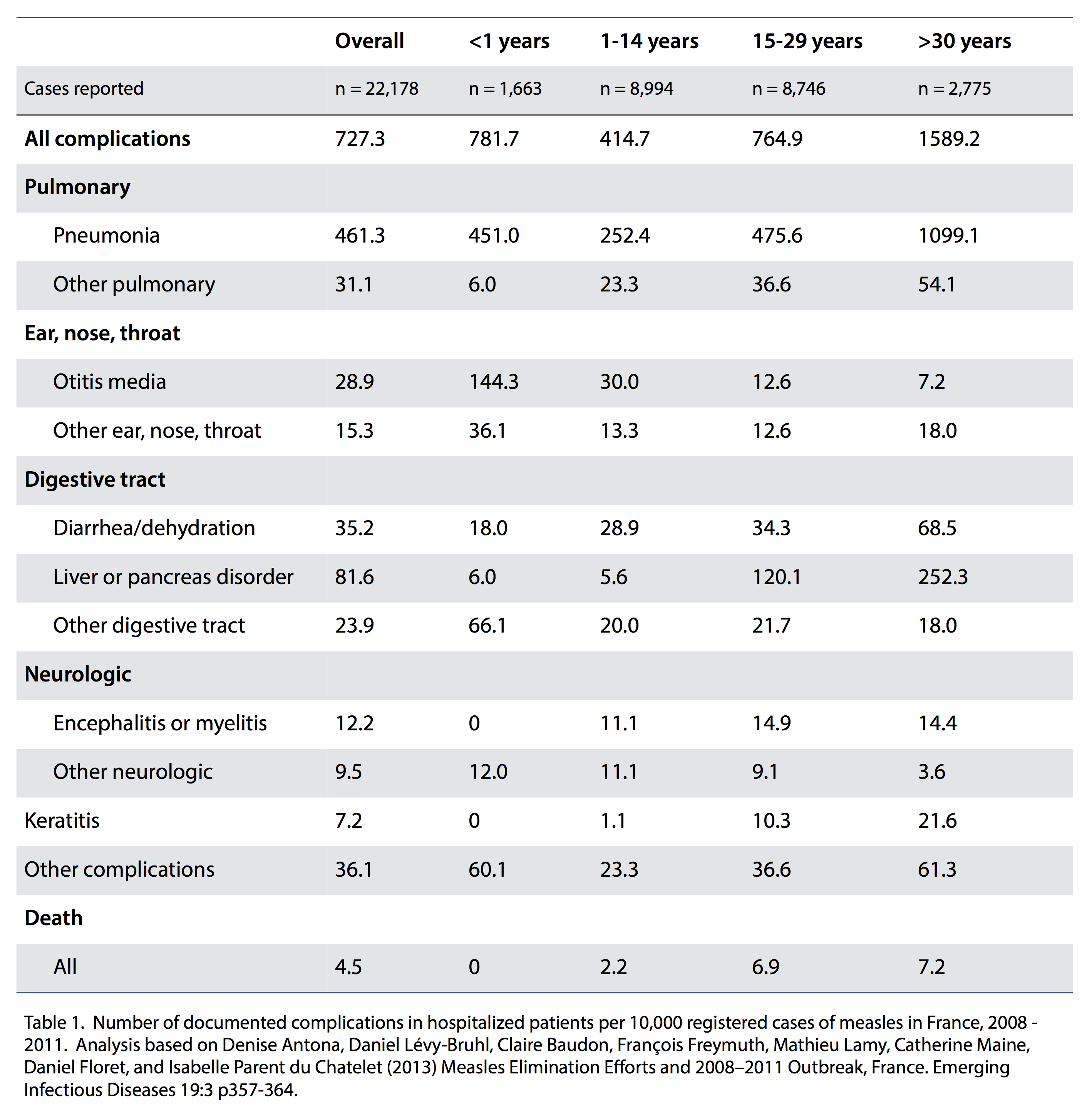
Focusing specifically on mortality, the overall rate was 4.5 deaths per 10,000 documented cases of measles. The rate was highest amongst individuals 30 years old or more (7.2 deaths per 10,000 documented cases), with those between 15-29 years old having a mortality rate of 6.9 per 10,000 documented infections. There were no deaths recorded amongst the 1,663 children under the age of one who were documented as contracting measles.
The paper’s authors also split the documented deaths between patients who were immunodeficient, and those who were not. Of the ten patients who died, one had congenital immunodeficiency and six had acquired immunodeficiency (e.g., Hodgkin’s lymphoma, Crohn’s disease, HIV, immunosuppressive treatment). In other words, only 3 out of the 10 deaths recorded were associated with non-immunocompromised individuals.
The overall mortality rate of around 4-5 deaths per 10,000 cases of measles for all individuals is slightly higher than the estimate based on historic US data. However, it doesn’t account for underreporting of measles infections, which the paper’s authors estimate at something over 50%.
Adjusting the data in table 1 by assuming only 50% of measles cases were reported gives the morbidity and mortality rates estimated in table 2 (below).
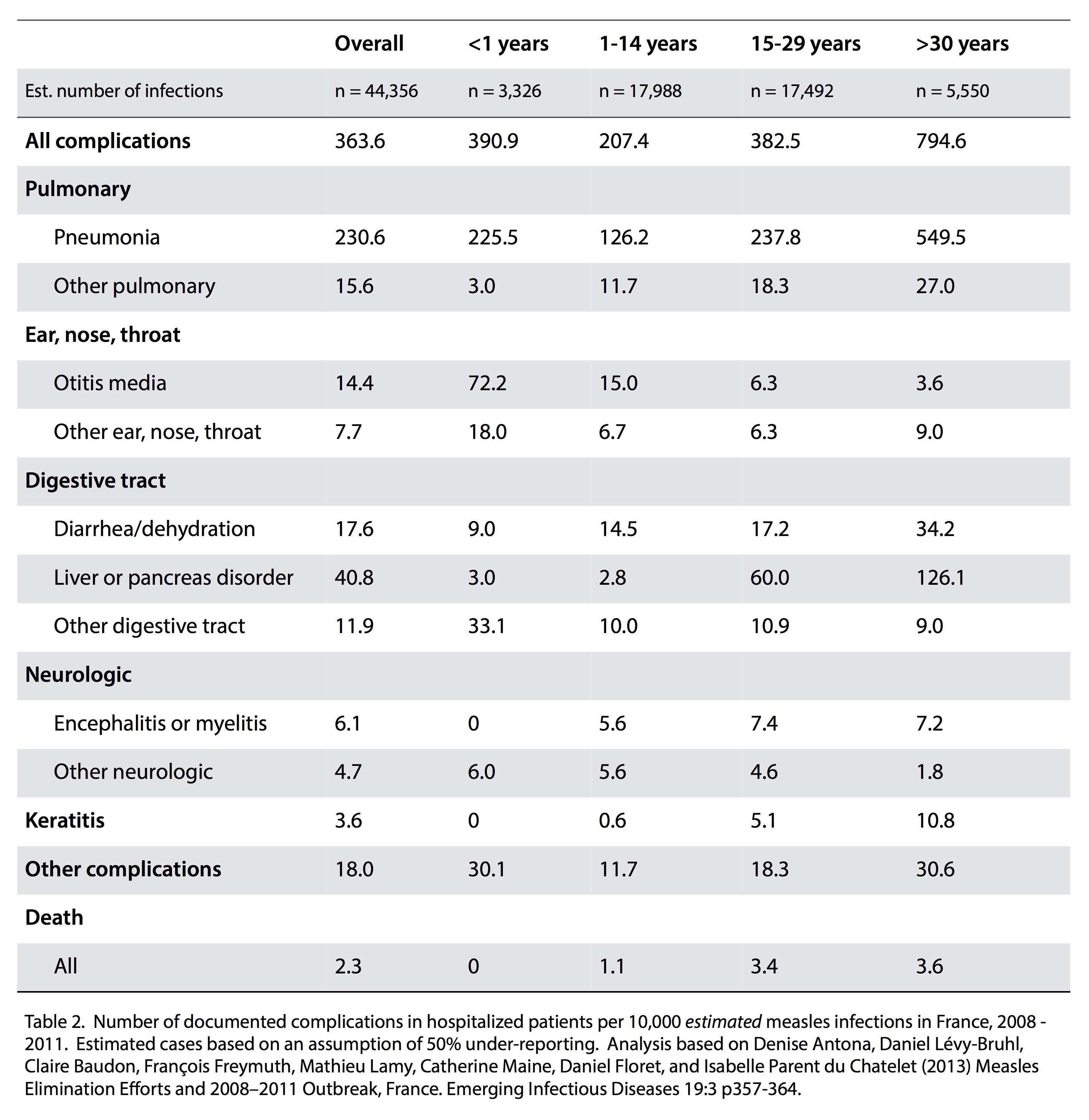
The overall mortality rate here is reduced to 2.3 deaths per 10,000 cases of measles. This value still reflects considerable uncertainty – there are likely to have been more non-fatal complications than were recorded with hospitalized patients for instance, meaning that estimated morbidity rates are probably substantially underestimated. However, it is less likely that there were substantially more measles-related deaths than were reported by Antona et al. It is also consistent with analysis of US data which suggest a mortality rate of the order of 1 in 10,000 for infected individuals.
That said, the morbidity and mortality rates presented here only tell part of the story. As was seen with the immunocompromised patients in the study, susceptible sub-populations may face a significantly greater risk from measles. This becomes a particular issue where there is an increasing probability of them coming into contact with infected individuals – as is the case where immunization isn’t widespread.
Nevertheless, the evidence from the French outbreak is strongly suggestive that, for infected individuals living in a developed economy with a robust healthcare system, the mortality rate is most likely less than 2-3 deaths per 10,000 cases.
I am a social scientist (medical sociologist/demographer) and I only have a passing knowledge of this but I’m bothered by the absolutist public health message surrounding vaccination risk as well as what seems to be the massaging of the message in presenting public health risks associated with the risk of specific infectious disease. I’ve been reading the 900 page IOM report on Vaccine Safety (and it is a work of scientific beauty) and their assessment is that for most of the vaccine-hypothesized adverse outcome pairs that they examined, the scientific evidence is insufficient to conclude that there are no adverse outcomes (which doesn’t mean there is an adverse effect just that we can’t reject the null). I also know from my own research as well as from peer reviewing manuscripts (it seems constantly) that epidemiologic observational studies are limited in their ability to detect adverse effects in small vulnerable subpopulations (especially if you don’t know where to look, as is arguably the case for conditions in which the etiology is poorly understood). And yet the public health (and more general public media) message is that the individual risk of an adverse event being causes by a vaccine is orders of magnitude smaller than the risk of suffering severe negative consquences from the disease (and backing that up by citing things like the 1-2 deaths per thousand you reference above). More broadly, in this highly polarized environment there seems to be a dogmatic assumption that anyone who questions the dominant public health message is an anti-science loon. My public health colleagues argue that putting a fuzzy (albeit more scientifically balanced and legitimate) message out there is too risky and does not serve the greater public good. But I fear that not being honest with the data (and scientific consensus from the Institute of Medicine) feeds into exactly the kind of conspiracy theories that perpetuate the problem of growing pockets of non-vaxxers. All of which is just to say that I think this is an important point that you have made, although my colleagues who work in public health would, I think, say that you shouldn’t be making it.
As a science-educated and concerned parent who’s researched this extensively, I’d like to thank you for your frank and informed comment. You hit the nail on the head when you wrote:
“But I fear that not being honest with the data (and scientific consensus from the Institute of Medicine) feeds into exactly the kind of conspiracy theories that perpetuate the problem of growing pockets of non-vaxxers.”
I often hear it’s “selfish” not to vaccinate but I believe it’s equally selfish to demand that others put their kids at risk for “the greater good” over sensationalized fears and beliefs.
Most selfish of all would be to not vaccinate while screaming that everyone else must vaccinate.
Any data of those that were vaccinated vs. non-vaccinated that contracted the measles? Find it very interesting that the older people were worse off that the babies, I always assumed that babies were at the top of the risk category.
There is some in the paper, but it’s not that clear – I’ll dig out what I can shortly
Kate,
From the Antona et al. paper:
“As the virus spread nationwide, the most affected areas were, as expected, those with the lowest vaccine coverage, mainly in southern France. However, even districts with >90% MMR1 coverage in toddlers were affected, confirming that a very high level of immunity is required for measles elimination”
…
“Overall, 80% of notified cases occurred in unvaccinated persons. … the ease that the virus had in spreading could by no means be explained by lower than expected vaccine effectiveness”
…
“Although vaccine coverage improved over time during the outbreak, our experience confirms that high coverage in children is insufficient to avoid the spread of measles virus, especially when catch-up vaccination in older cohorts remains insufficient.”
i.e. the vaccine was highly effective, but not 100% effective, and unvaccinated toddlers were especially at risk of contracting the disease, even when there were high vaccination rates within their community, suggesting that higher-still vaccination rates are needed for strong herd immunity.
Regarding the statistics for those with compromised immune systems:
Do we even GIVE those people vaccinations? I thought we did not…just trying to imagine the whole picture, here.
Another statistic that seems not to surface: What becomes of those who have actually had a case of the measles once in their lifetime, when such an outbreak occurs? Where do they fit in these data? Do we vaccinate them? Do they again catch measles, or are they more immune than others? And what does that say about their ability, later, to fight off potentially fatal complications?
All important questions – and of course, mortality rate only tells part of a larger story. No, immunocompromised individuals will generally not be vaccinated, meaning that there is an even greater need for those who are healthy to be vaccinated in order to protect the vulnerable.
Yes, we do. I have a primary autoimmune disease, antibody deficiency. I need herd vaccinations. Ive actually taken the rubella vaccinations three times and cant get immunity from it. PIDD can vary though and some people should not take as they contract the disease. The immune system is very complex and not fully understood.
oops “a pressing pubic health issue”,
1. What are the risks from receiving the vaccine:
a. are the measured risks for the vaccines, measured on manufactured product as delivered to
patients(as opposed to samples submitted for test,)?
b. do the measured risks include risks from the effects of adjuvants, and if so what is the break
down of risk associated with the various ingredients in a vaccine?
c What do the studies or what can the studies say about any possible relationship between vaccines and auto-immune diseases?
d. Are there any studies that characterize the risks between vaccines and long term effects
(studies that could show show negative outcomes if they would occur after 3, 5, 10, or 15 years)?
e. What are the risks of being infected with viruses from various vaccines, such as SV4 for example, the polio vaccine virus?
Thank you for your honest and thorough analysis. As a concerned mother I found the often quoted 1/1,000 didn’t seem quite right and would then find myself not trusting the final message. This is the type of reporting I would like to see in the mainstream media.
Kristi: Can you post a link to the 900-page tome you reference in your comment above? I’d like to read it. Thanks.
I’d love to hear your thoughts. You have to create an account to download it but doing so is free: https://www.iom.edu/Reports/2011/Adverse-Effects-of-Vaccines-Evidence-and-Causality.aspx